For anyone who is “vitamined-out” — ponder that the most important theme is not just about personally avoiding hospitalization, it’s Where the hell are our publicly funded universities? Does the Minister for Health serve the People, or Pfizer…
————————————–
Vitamin A was allegedly once called “ “the anti-infective vitamin” — a snappy title which didn’t stick with any biochem student beyond the end of the sentence. But it’s needed for your immune system to function normally, so it seems sort of obvious to ask “what if” we don’t have enough. Could taking more prevent people catching Covid or ending up in hospital, or dead?
As always, research in prevention and prophylaxis is a wasteland in the the Modern West. No one can profit from it and indeed if everyone got enough it could harm the prospects of shareholders of Pharmaceutical firms and Hospitals. But it appears we definitely don’t want to be short of it. About three quarters of people who end up in the severe ward of Covid hospitals were deficient.
Imagine a Minister of Health who embarked on a program to raise awareness, test and give out free supplements? Lordy! It might reduce hospital loads in a week?
Vitamin A makes our bones stronger, reduces wrinkles, may prevent cancer and stops us going blind. But it’s possible to eat too much — especially if we dine out on polar bear livers or sled dogs. Seriously, overdosing for pregnant women causes birth defects and trouble for anyone who really overdoes it.
Sighs of Vitamin A deficiencyinclude dry skin, excsma, dry eyes, night blindness, infertility, chest infections, poor would healing, and acne. Though all of these can be caused by other things too. People who are anaemic and people with inflammatory bowel disease, fibrosis, liver trouble or pancreatitis are more likely to be deficient.
Our immune systems can’t work without it
Our white blood cells that catch some booty (like body-parts of germs) will turn up to show it off, and when they do they’ll ooze versions of Vitamin A which induces other immune cells to respond to their prize and mature and proliferate. Vitamin A also manages to mobilize iron stocks to fill up the haemoglobulin molecules in baby red blood cells, something that makes them both red, and useful. It’s easy to imagine how extra red blood cells, and thus oxygen carrying capacity might be handy when dealing with a disease notorious for inducing low blood oxygen.
Vitamin A comes in meat, eggs and milk, but precursors (the carotenes) are found in leafy and colorful vegetables like spinach and carrots, so even vegetarians, in theory, ought to be getting enough of the building blocks so their livers can finish the job.
But a study in Spain showed that the sickest people with Covid were often the ones that were deficient. Three quarters of those admitted to hospital were deficient in zinc and Vitamin D, but nearly as many, 72%, were deficient in Vitamin A. And 42% were low in B6 (see Tomasa-Irriguible).
The problem with that kind of study is that we can’t be sure that the disease didn’t create the deficiency, and that the sickest people drained away their A and zinc in the process of getting sick. But from other studies we already know that Vitamin A is anti-inflammatory, as well as helping promote immunity. (Li et al) And that backing up a truck and giving super massive doses of 200,000IU to Covid patients appeared to save about two thirds of them from ending up with a severe disease. (see Al-Sumiadai).
Naturally, there aren’t many big good definitive studies in the West. We throw billions at patentable experiments, and our public universities, but no one is that interested in the ten-cent-nutrients that might reduce deaths by half. Though one large prospective study in the UK followed 15,000 people and found people taking Vitamin A and selenium supplements were quite a lot less likely to get a positive Covid result — odds were reduced by about 60% and 80%. (Holt et al).
One small Iranian study gave a mixed bag of vitamins to 30 patients and estimates the risk of hospitalization was 40% less, and the risk of death was 90%less compared with 30 “controls”. (It says something that we keep coming back to small Iranian studies, doesn’t it?)
5,000 IU vitamin A daily, 600,000 IU vitamin D once, 300 IU of vitamin E twice a day, 500 mg vitamin C four times a day, and one ampule daily of B vitamins [thiamine nitrate [B1] 3.1 mg, sodium riboflavin phosphate 4.9 mg (corresponding to vitamin B2 3.6 mg), nicotinamide [B3] 40 mg, pyridoxine hydrochloride [B5] 4.9 mg (corresponding to vitamin B6 4.0 mg), sodium pantothenate [B6] 16.5 mg (corresponding to pantothenic acid 15 mg), sodium ascorbate 113 mg (corresponding to vitamin C 100 mg), biotin 60 μg, folic acid 400 μg, and cyanocobalamin [B12] 5 μg]. IRCT20200319046819N [1].
If there was a sign of a major problem with energy policy it might look just like this:
In the EU for most of the last ten years gas prices were €20. Last week they spiked to €180. Prices have come down in the last few days as a flotilla of 15 US tankers crosses the Atlantic to rescue the EU and some Russian troops departed from the border near Ukraine.
It’s heartwarming to see the US tankers on the way:
US Tankers headed for EU
No sign the EU governments get the message:
What will it take? The Netherlands announced that they will limit coal stations and pay them not to produce electricity most of the time in the hope of stopping floods and droughts:
Dutch coal-fired power stations may not operate at more than 35% of their maximum capacity in the coming years. “In the short term, this will lead to a significant reduction in CO2 emissions at coal-fired power stations of approximately 6-7 megatons,” the Ministry of Economic Affairs and Climate (EZK) reported on Wednesday.
The owners of the coal-fired power stations are financially compensated by the government for the lost income from the reduced electricity production up to and including 2024.
In Germany, the sabotage continues: 11 nuclear reactors have been shut, three are about to. The last three will go next year:
Rarely has a country worked so hard to make itself vulnerable.
Ten years ago 17 nuclear reactors produced about a quarter of Germany’s electricity, but the 2011 Fukushima accident prompted former Chancellor Angela Merkel to phase out nuclear. Six reactors remain: Three will close this month, with the remaining three ceasing operations next year. It’s hard to think of a more self-defeating policy on economic, climate and geopolitical grounds.
German one-year forward electricity prices have hit €300 per megawatt hour. For comparison, the 2010 to 2020 average was under €50 per megawatt hour.
Coal was Germany’s top energy source in the first half of 2021.
How big is this crisis? Even in France, where nuclear power is running, the energy price spikes are causing major industries to shut down:
With energy costs spiking to fresh records day after day, financial strain is mounting for industries including metals and fertilizers. Aluminium Dunkerque Industries France, Europe’s top smelter of the metal, curbed output in the past two weeks.
Trafigura’s Nyrstar will pause zinc production in France in early January and Romanian fertilizer maker Azomures temporarily halted activity.
“We’re seeing an existential crisis of the European aluminum industry and other metals-smelting industries that are power intensive,” Mark Hansen, head of metals trader Concord Resources, said. “It’s not always so easy to get these businesses back in operation”
Meanwhile, spare a thought for the people in Kosovo who were suffering through 2 hour rolling blackouts in the lead up to Christmas. Lest we forget who is responsible:
Javier Blas: Dec 24 As Kosovo homes go dark with rolling blackouts from today, just before Christmas, let’s remember that in 2018 the World Bank pulled the plug on a project to build a new coal-fired power plant in the country. The same coal Germany and the US burns today.
It takes a really Big Government to do Really Stupid Things.
Absolutely no one who writes for newspapers has any idea of why Covid may have almost completely disappeared from Japan since the sudden Delta wave in August. The trajectory collapsed on August 25th and vaccines don’t explain it.
Call it the hunt for a potential “X factor,” such as genetics, that may explain the trend and inform how Japan could deal with the next wave. While the new highly transmissible Omicron variant has appeared in the country and experts suspect there is already some community spread, the overall transmission rate of the virus and coronavirus-related deaths in Japan have remained low. “
” “Honestly, we do not know the exact reason behind the sudden drop in COVID deaths in Japan,” said Taro Yamamoto, professor of global health at Nagasaki University’s Institute of Tropical Medicine. “
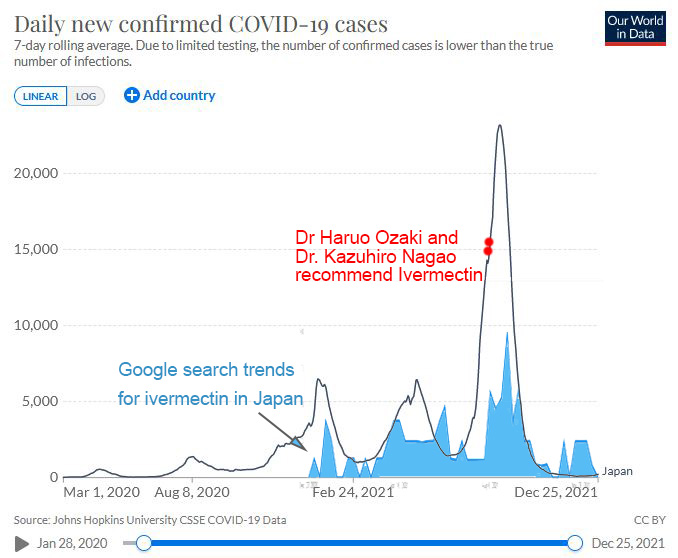
There is no mention of the-drug-that-shall-not-be-named — Voldermectin. But on August 13th as the third major wave was running out of control, a high ranking doctor in Tokyo recommended doctors use ivermectin. Dr. Haruo Ozaki, the Chairman of the Tokyo Medical Association said it was time for doctors to give patients information on ivermectin “and get permission to use it”. Around the same time, possibly on August 10, another doctor, Dr. Kazuhiro Nagao was seen on a Japanese television show calling ivermectin “a silver bullet” and describing how he’d treated 500 patients with ivermectin and they “all felt better the next day”. (See below). The peak of daily cases in Japan was two weeks later on August 25th, 2021.
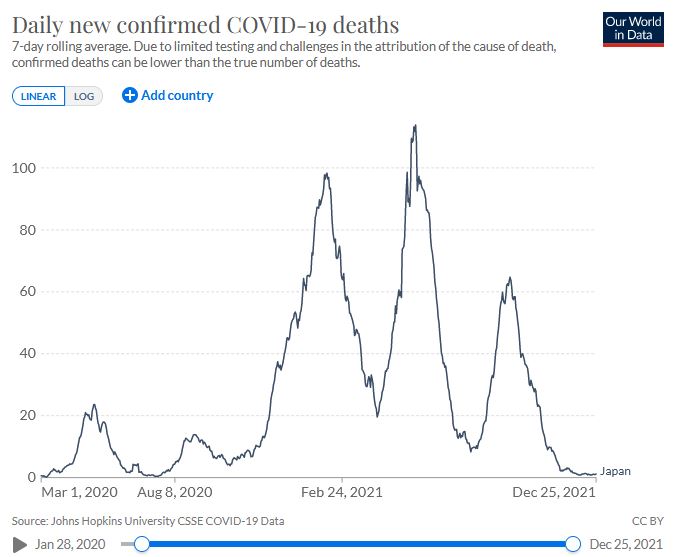
In Japan, the third major peak was more than four times larger than previous peaks.
Things were looking pretty bleak in August during the post Olympic spike of cases for a while there were more than 20,000 new cases every day. Then, “a miracle” occurred, and now in a population of 126 million the current daily cases across the whole of Japan amount to a very small, 200 per day.
Japanese cases of Covid plummet as people search for ivermectin.
So the extraordinary turning point in cases starts 2 weeks after two Japanese doctors recommended ivermectin and searches for the word “ivermectin” in Japan became more popular than ever.
Searches for the word “ivermectin” peaked in Japan on August 29th – September 4th. | Source
But also watch the Japanese Doctor Kazuhiro Nagao director of the Nagao clinic on TV in August talking about how we “give Ivermectin to everyone who wants it”, on the “same day” they test positive. “They feel better the next day”. Watch the expression on the interviewer in the last second where he asks Dr Nagao how many of his 500 patients got worse afterwards, and Dr Nagao says “None.” (If you can’t see the video below try another browser!)
Dr. Kazuhiro Nagao on Japanese TV saying he’s used #ivermectin as early treatment for over 500 covid patients with practically 100% success rate. Asks for nationwide use.
Dr. Nagao is director of the Nagao Clinic and a university professor.
Google translate is struggling. But the good doctor said with “the silver bullet” ivermectin Covid should be reclassified to just a seasonal flu.
Dr. Nagao recommends that corona, which is currently classified as Class 2, be treated as Class 5, which is the same as seasonal influenza. By lowering the price, “early diagnosis and immediate treatment by a practitioner is possible = prevention of aggravation” “Practitioners directly request for those who need immediate hospitalization = no time lag” “Health observation of close contacts, no need to allocate hospitalization destinations” “= Eliminate the collapse of the health center” and three merits are mentioned. That’s important. ” He also said, “There is a silver bullet called ivermectin that anyone can use. It is a drug that is usually used for the treatment of scabies. It will be distributed to all people.” He also proposed a “suganomectin” system that is comparable to “abenomask.” On top of that, Dr. Nagao said, “If I make a mistake, I will take responsibility and quit the doctor.” It only looks like it’s waiting for it to change. If you treat it early, it’s over. No one I’m seeing is dead.
All of these quotes are extremely hard to find now, so thanks to readers who sent in these links (see the hat tips at the end). I keep all those emails.
Explaining miracles with magical thinking
A search for “Ivermectin in Japan” now though will turn up 50 news stories categorically saying that “No, Ivermectin Did Not Help Japan Bring Down Covid-19 Coronavirus Delta Surge”. Apparently the fall is a complete mystery, but was absolutely, definitely not due to ivermectin.
It might be because Japanese people wear masks, though they did that through all the other peaks too and it didn’t stop the rise, nor cause a sharp fall. It might be because Japanese people have a rare gene called APOBEC3A, though they probably had that gene in waves 1 and 2 as well and there were no miracles then. It might be because the Delta virus in Japan mutated itself out of existence. That creative theory centres on the A394V mutation, which occurs on nsp14 – a viral gene that checks for errors. The idea is that if nsp14 is faulty the virus might just make such bad baby viruses that they stop infecting people. It doesn’t really sit well with natural selection. Somehow the virus was incredibly fertile til August 25th, then the superspreading dominant Delta variant was somehow outcompeted by a baby that couldn’t make good copies of itself. Which sort of begs the question of why one of the other offspring-of-delta didn’t just take over and outcompete the dud baby. And as John Campbell points out, that same gene occurred in the virus in 24 other countries. It can be found in strains AY.1 AY.3 AY.4 AY.5 AY.6 AY.7 and AY.12 strains. No miracles.
Vaccinations don’t explain it
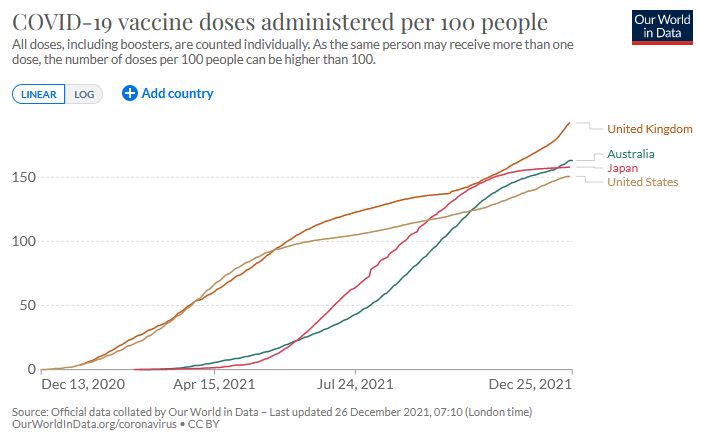
At the point when the caseload peaked and suddenly flipped, only 44% of Japanese people were fully vaccinated. It’s hard to believe that reaching the number 45% the next day somehow triggered the miracle.
Not to mention that many other countries vaccinated a similar number of people but they didn’t crush Covid.
All four nations followed similarish vaccination trends but had very different outcomes. source: OWID
One eighth of the death rate?
The third big peak in Japan was really quite remarkable. Despite having four times the caseload of all previous peaks, the deaths per day were half as high as the first and second peaks, even though the biggest peak was almost solely due to the deadlier Delta variant. The second peak was 90% Alpha variant (the UK variant). Mortality in the UK, Scotland and Canada was worse for Delta.
So some of the reduction in death rates is due to the vaccination program, but when half the nation wasn’t vaccinated, it doesn’t make sense that the death rates would fall by a factor of eight.
Despite the third major peak being the highest case load in Japan, and due to the Delta variant Covid deaths per day in Japan were half the previous peak.
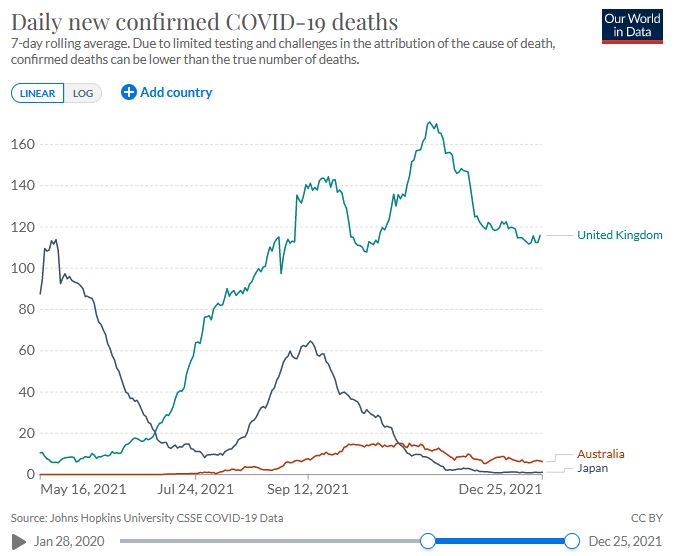
And if vaccinations produced miracles it would work in other nations too. However, Australia has one fifth the population but six times the deaths. The UK has half the population of Japan but on a daily basis, this week, 100 times the deaths.
According to OWID, currently 71% in Australia are fully vaccinated, 69% of the UK, and 78% of Japan. Clearly the vaccination rate doesn’t explain the massive discrepancies in death rates.
The UK has half the population of Japan but 100 times the deaths. | Source: OWID
…
Apparently, Ivermectin is still being used in Japan and people are not happy
BY OSAMU TSUKIMORI , Dec 21, 2021, Japan Times
Authorities have flagged concerns over scores of messages posted on websites for agents that import drugs into Japan from those who have mail ordered the anti-parasite drug ivermectin.
“I just received the package and, to prevent (coronavirus) infection, I’m going to take it from today,” a 52-year-old man wrote in a message posted in September.
There are agents in Japan that order in ivermectin?
So the bottom line is that officially in Japan, the vaccines are being rolled out and boosted, like everywhere else in the modern world. But unofficially, doctors in Japan are speaking out publicly saying that ivermectin works, and people are ordering it in from India. The government of Japan doesn’t need to mandate or approve ivermectin use. Word of mouth will do it, especially when lives are on the line.
h/t Richard Kleenman, David B, Panda, David Archibald, Scott of the Pacific. David E.
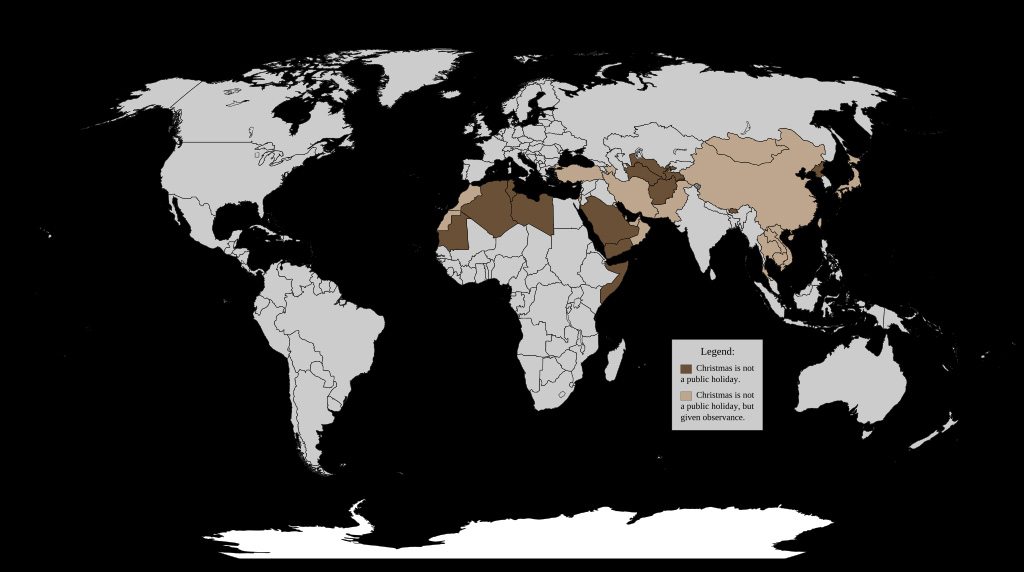
What makes this map so apt, especially today, is because these are the countries that don’t celebrate Christmas (in brown). It’s a testament to how far the spirit of Christmas has spread.
…
Lighter brown countries (China, Turkey, Saudi Arabia) don’t have a public holiday but are described as “giving observance”.
There is a crisis. People are getting stuck for days extra in hospitals and even dying because of nutrient deficiencies that we could easily solve.
A new study from Istanbul shows that even if we negligently fail to correct Vitamin D deficiencies before people get sick, we can still save half of the ones who might die with a cheap vitamin, pumped in hospital for about 1/5000th of the daily cost of an ICU bed.
The mortality rate in the unsupplemented group from 2020 was 11%, but in the supplemented group in 2021 it was 5.5%. Imagine what the mortality rate might be if these people weren’t deficient in the first place?
The study shows us that there is a causal connection between low Vitamin D and more severe Covid. It also shows what a train wreck our medical systems are. For the price of a few dollars we can free up a lot of hospital beds and stop a lot of deaths, and we’ve known this might be the case since the beginning, and we’re still not doing it? The incentives are so screwed in our healthcare systems that we’re waiting for doctors in Turkey to do the trials we should have done in February 2020?
Don’t wait til you catch Covid to get your D3 levels tested.
Sort it out now, and supplement if you need it. And aim for the higher end of the normal spectrum. (And take Vitamin K2 as well, though NOT without doc approval if you are on anticoagulants like warfarin, see comments below).
This new study enrolled 163 people admitted to hospital with Covid who had low to moderate Vitamin D levels (less than 30 ng/ml.) About two thirds of them were then given some whopper combinations of Vitamin D which started with 100,000 IU on Day One, and then continued for up to 7 days with lower doses that ranged from 2,000IU a day up to 100,000IU.
So all these patients were given supersized cumulative Vitamin D doses over the next week of between 224,000IU up to 500,000IU. Staff did blood tests on Day 7 and 14 to make sure they weren’t overdoing it. They compared the new supplemented patients with the survival rates of 867 people admitted to the hospital a year before, whose Vitamin D status was known and who didn’t have comorbidities. It’s not ideal that the earlier group probably were sick with a different variant — the original WuFlu. But random controlled trials seem so cruel when we already have a pretty good idea of what works.
Medico’s will find the study interesting because it assesses a lot of blood markers. Vitamin D levels were a better predictor of hospitalization than things like diabetes and high blood pressure.
We hear all about the “co-morbidity risks” in the media, but Vitamin D appears to be more important.
People who had no comorbidities, who should have been better off, were twice as likely to need a long hospital stay as people with comorbidities who also got Vitamin D treatment in hospital. That applies to people who had Vitamin D in the moderate category — lower than 30 ng/mL.
UPDATE: This is a sticky post. New posts are appearing below.
So here’s wishing you a Merry Christmas, and asking if you wouldn’t mind helping out. We’re in a kind of guerrilla warfare against a world of vested interests.
As always, due to legal froufrou, donors can buy however many “units of emergency chocolate” they can spare in AUD, CAD, EUR, GBP, NZD or USD.
Thank you. In a year when Twitter cancelled the US President and the oldest masthead in America, somehow I was able to keep writing. Largely because many readers chip in to cover the costs. In the cancel culture era, when institutions became weapons, lone bloggers living off donations were able to say things even most newspapers found unsayable. Real freedom is writing with no large sponsor, no major advertiser, no platform to toss us off, no editor to boss us around, and no committee to answer to. The government can’t take away a grant it never gave me, or a permit I don’t need. Cancel culture can’t scare away advertisers or cut nebulous revenue-streams.
In more news you can use before Christmas, here’s another cheap easy way to put the brakes on Covid — this time with the antiseptic Povidone-Iodine (PVP).
While Carrageenan can clog up the virus in the passages behind your nose, it doesn’t necessarily do much to stop the virus replicating in your mouth and throat. But a regular swish or a sniff with Povidone-iodine can reduce the viral load to nothing in a matter of 15 to 30 seconds. Note, you’re supposed to spit it out again, not drink it and make sure to use a very dilute solution.
Saliva can contain as many as 100 million infectious copies of Covid per ml, so the aim here is to reduce the number drastically every four hours. It’ll reduce the risk of you infecting people around you, and probably help buy yourself time to fight back against the virus.
Patrick J. Lynch, medical illustrator
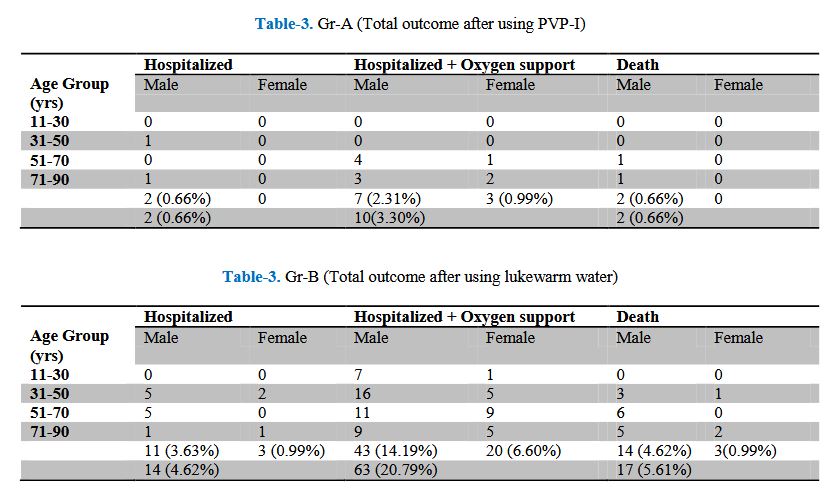
Between February and August last year Choudhury et al enrolled 600 people in Bangladesh. Half were asked to use a 1% povidone iodine solution to gargle, use in nasal drops and eye drops. They were asked to do this every 4 hours for 4 weeks, which sounds like a chore, but is nicer than going to hospital. The other half did the same thing but only with lukewarm water. Since nasal rinsing is sometimes claimed to be useful, even the placebo arm may have got some benefit. But the difference was still impressive.
Only 3.3% of the group that used Povidone-Iodine ended up in hospital, while nearly 21% of the plain “water washers” did. Only 2 people died in the treatment group, but 17 people did in the control group.
Randomised controlled trials are useful, but brutal. Perhaps 15 people might not be dead now if they had been randomly assigned to the other group.
The bottom row is the total male plus female.
This is good for everyone except Pharmaceutical companies selling vaccines and treatments.
So the patients those who used 1% PVP I have minimum mortality, morbidity and occupying minimum number of hospital bed causing less burden to health and financial sector of Bangladesh in COVID-19 pandemic situation.
Why can’t Australia do studies like this? Perhaps because we’re rich enough to be a market-worth-capturing?
Chopra et al reviews the situation from a dentists point of view. Dentists are at high risk of catching covid, especially for some procedures, so Dental associations are keen to give patients a mouthwash and rinse before treatment so people don’t infect their dentist.
The CDC recommends preprocedural rinsing with antimicrobial rinses such as chlorhexidine gluconate, essential oils, PVP-I, or cetylpyridinium chloride. PVP-I is safe for use in the oral and nasal cavities at concentrations up to 1.25% [21]. In the absence of any commercially available preparations for routine dental use during the COVID-19 pandemic, it is advised to dilute 10% PVP-I by 1:20 and mix 0.5cc of the diluted PVP-I solution with 9.5cc of sterile saline or sterile water for routine clinical use
Chopra tested four products of PVP-I for a contact time of 30 s for virucidal activity,
a. Antiseptic solution (PVP-I 10%)
b. Skin cleanser (PVP-I 7.5%)
c. Gargle and mouth wash (PVP-I 1%)
d. Throat spray (PVP-I 0.45%)
They concluded: “All products of PVP-I inactivated the virus by ≥99.99% which corresponded to ≥4log10 reduction of virus titre, within 30 s of contact”
So even the half-a-percent solution still killed 9,999 viruses out of 10,000 and with only 30 seconds of swishing. Not bad.
Obviously, it wouldn’t be good to drink antiseptic and it is possible to overdo it.
Again, the aim with mouthwashes or nasal sprays and eye drops is to whack the viral replication in the early days, and thwart the virus. An antiseptic won’t kill every germ — especially not the ones hiding inside your cells, but it will buy your B and T cells time to figure out the best plan of attack, and stop you infecting everyone around you.
If only the vaccines worked this well?
ht to Vicki, redress, OldOzzie, Dipole,Nabrid Obcsje
Chopra, (2021) Can povidone iodine gargle/mouthrinse inactivate SARS-CoV-2 and decrease the risk of nosocomial and community transmission during the COVID-19 pandemic? An evidence-based update,Japanese Dental Science Review, Volume 57, November 2021, Pages 39-45.
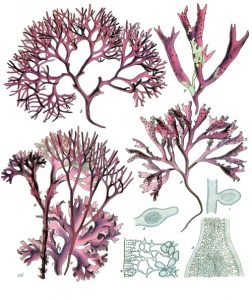
More than one hundred years ago the Irish believed an extract from a red seaweed could cure sick cows, and humans with colds and flu’s. In terms of early treatment modern medical science is slowly catching up with 19th Century farmers. In a small trial this year medical workers were 80% less likely to catch Covid if they were using a nasal spray with the “Irish Moss” carrageenan extract. It’s only a case of 2 out of 200 catching Covid in the test group, compared to 10 out of 200 in the placebo group, so the “80%” is a rubbery number, but it was a randomized control trial, and there are other lab test results which suggest the effect is real.
And because we recently figured out it was useful against common colds and influenza’s, nasal sprays with this common safe food additive are already on sale at the Chemist. So you can pop in and get one before Christmas Parties.
Carrageenan or “Irish Moss” is a polysaccaride gel from a red seaweed. It works by gumming things up for quite a few viruses — basically getting in the way and trapping them in the gel. The idea is to squirt it up your nose three or four times a day to make it hard for a virus to get in. Not as much fun as a glass of champers, but more fun than a head cold.
Carrageenan is a food additive, and it’s so safe a 70kg person could eat half a kilo of it a day “with no adverse effects”. So it’s safer than table salt. We’ve known since the 1980s carrageenan’s been useful in the lab against influenza viruses, coronavirus OC43, rhinoviruses, and coxsackievirus. Which is why it’s been put into commercial nasal sprays. One here in Australia is called Flo Travel, aimed at travellers sitting on planes, but there will be others. Look for iota-Carrageenan in the ingredients.
In Ireland it’s use goes back to about 400AD, but in places like China, about 14,000 years. Currently carrageenan is added as a thickener to things like icecreams.
Seriously — a nasal spray?
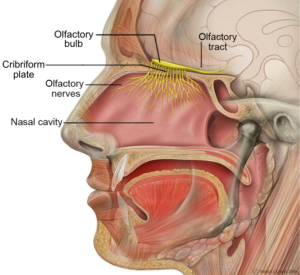
Two years ago I would have said “bollocks.” I assumed that a squirt up the nose wouldn’t stop all the virions and it seemed an exercise in futility. It only takes one virion to get through the gates and it will make 1000 babies. By the time one baby virus gets into your lungs, the nasal squirty spray will be irrelevant. But the vast area at the back of your nose and mouth is often the first spot an airborne virus latches onto. There is something like one square meter of surface area behind our noses for viruses to romp in:
The nasal cavity has a volume of between 15 and 19 ml, and a macroscopic surface area of 150–180 cm2, however the presence of microstructures such as microvilli on the columnar cells drastically increase this surface area to around 96,000 cm2
And if the gel spray misses the first virus, it can still be there to catch a lot of the baby-viruses as they leak out of the hijacked cell. That means a big reduction in viral load, which means less chance of the virus getting into your lungs, or your digestive tract, and less chance of breathing it out and infecting a friend. It also means you can slow the rampant exponential phase and buy your immune system time to find the right key and make the right weapons. In the arms race of exponential expansion, extra time at the start is a big advantage.
The back of your nose is the new frontier
Patrick J. Lynch, medical illustrator
It’s not just nasal sprays, there are also throat gargles, nasal washes, and all kinds of ways to killing or flush virions out at the start. The Docs in Spain with the remarkable 100% survival rate used nasal washes with bicarb. I’ll write more on these other strategies soon.
So, spray away before events, you’re less likely to catch Covid and quite a few other viruses, and if you do catch something, then it’ll still likely reduce the length of time you are ill.
It’s just another early treatment that our Minister for Health forgot to mention
The big question is, like always, we’ve clearly known this was a reasonable possibility since the very beginning of the Covid epidemic, yet here we are, billions of dollars worth of lockdowns and five million dead people later, and the giant industrial medical complex didn’t think it was worth mentioning. No “awareness” campaigns, no free samples from every GP. No government advertising, no news spots.
It’s yet another cheap and safe way to slow the virus, but still have more normal lives.
People using carrageenan got better faster.
Click to enlarge.
In another bonus, not only does it reduce the length of long colds, it also reduces the recurrence of them.
Say it ain’t so. The Australian government appears to putting roadblocks in the way of an Australian vaccine. Does Scott Morrison and the TGA serve Australians or Pfizer?
” COVAX-19 is the first recombinant protein COVID-19 vaccine to be authorised anywhere in the world, beating Novavax to this key milestone. * “
The TGA should be abolished if it serves foreign corporate interests. That’s Scott Morrison’s call.
Even if you don’t want a vaccine at all, it’s in all our interests to develop local medical suppliers, real competition, and to give free citizens a free choice.
So imagine you live in a house with six people and you elect one of them to do a deal with the chemist to supply the whole house drugs. When you get back from Hardware Mart, he’s done the deal, but you can’t see the contract, or the trial data, you don’t know what it costs, or how long it lasts, but the money will be auto-drawn in unmarked tranches until such time as it is not. Then you find out you have to take the drug, or you won’t be allowed in the kitchen.
It’s a crime in the house, but ok for a nation?
There have been several allegedly leaked contracts with Pfizer, one from Albania, and others from Brazil and South America. They all make extraordinary claims, they can’t be backed up. They might all be fakes but here’s the thing, we don’t know they’re fake because we can’t see the real thing.
Is Pfizer the bully that asked Argentina to accept all liability on its behalf and put its bank reserves, military bases and embassies at stake as collateral? “That the rules of the land don’t apply”. That the government may not discuss anything to do with the contract or Pfizer without asking permission from Pfizer.
Who can tell?
“It’s a private company muzzling a government”
Why the secrecy?
Try to imagine what possible benefit accrues to the whole house from signing deals on their behalf that most inhabitants can’t see? Perhaps the crooks, I mean chemists, sold it to their guy “real cheap” and it was cheaper than all the neighbors, so the chemist doesn’t want the other houses to know they paid more. If you’ll believe that…
We don’t know if the PM or President signed away Fort Knox, or London Bridge, or their own right to discuss problems with the vaccines or if they paid twice the price, agreed to nobble competitors, or let Pfizer steal intellectual property.
Apparently, in terror, all our democratically elected leaders signed away the ranch, our ranch, perhaps dreading headlines like “Thousands Dead because PM used home made Vax.”
1. Pfizer Reserves the Right to Silence Governments
…neither Pfizer nor the U.S. government can make “any public announcement concerning the existence, subject matter or terms of this Agreement, the transactions contemplated by it, or the relationship between the Pfizer and the Government hereunder, without the prior written consent of the other.”[28]e Governments.
4. Private Arbitrators, not Public Courts, Decide Disputes in
What happens if the United Kingdom cannot resolve a contractual dispute with Pfizer? A secret panel of three private arbitrators—not a U.K court—is empowered under the contract to make the final decision.[41] The arbitration is conducted under the Rules of Arbitration of the International Chamber of Commerce (ICC). Both parties are required to keep everything secret
5. Pfizer Can Go After State Assets.
Pfizer required Brazil, Chile, Colombia, the Dominican Republic, and Peru to waive sovereign immunity.[50] In the case of Brazil, Chile and Colombia, for example, the government “expressly and irrevocably waives any right of immunity which either it or its assets may have or acquire in the future” to enforce any arbitration award (emphasis added).[51] For Brazil, Chile, Colombia, and the Dominican Republic, this includes “immunity against precautionary seizure of any of its assets.”[52]
Everything about what it means to be a democracy, and what Rule of Law means, and the whole Magna Carta deal has apparently ended?
In March 2020 a group of doctors working in nursing homes in Toledo, Spain faced a new pandemic with no effective treatment plan. They figured out their own protocol as best they could with what can only be described as freakish success. In nearby Albacete when Covid struck 1084 nursing home residents, 303 of them died, a 28% fatality rate. But in Toledo, of the 90 patients in nursing homes under Doctor Blanco’s care, only 6 died, and they all died before the team figured out their own new treatment plan. Of the 84 residents who were then treated with antihistamines like Polaramine, all 84 would make it. Every single one, even though their mean age was 85.
It seems too good to be true. Antihistamines are used to calm an overactive immune system (itchy, sneezes and runny noses) but they are not known for their anti-viral activity, though it turns there is some.
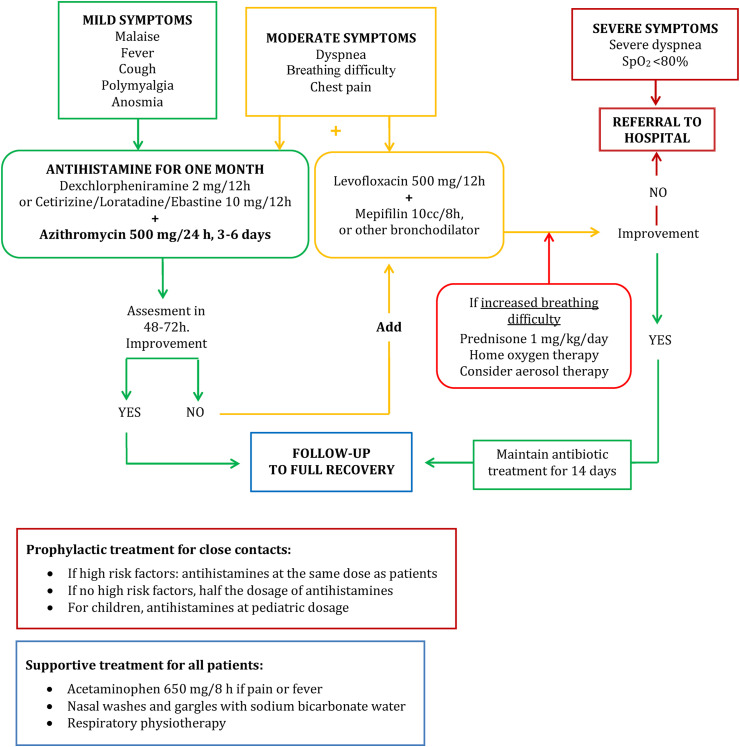
And while the antihistamines are possibly very helpful, the whole treatment protocol was so much more, and also included nasal washes, antibiotics, and prednisone, as well as something called “respiratory physiotherapy”. Somehow these doctors, saints or geniuses, had figured out a combination that worked, and there was no obvious reason why it should be treated like a lucky freak and ignored while millions literally died, yet that of course is precisely what happened.
Another research group in Spain studied nearly 80,000 people to see whether there were patterns in who got infected the most often. Only a few things ended up being significant and one of those was histamine use. People using antihistamines were half as likely to catch covid. (Vila-Córcoles).
But make no mistake, their treatment plan was a lot more than just Polaramine, and the antibiotics and nasal washes would all be important too.
For example, azithromycin works against a lot of viruses:
Numerous studies describe a possible antiviral activity of azithromycin against viruses as diverse as influenza viruses (Orthomyxoviridae), rhinovirus (Picornaviridae) [10], respiratory syncytial virus (Paramyxoviridae) and zika (Flaviviridae) [11]. Tran et al.[12] demonstrated the possible mechanism of antiviral action of azithromycin that blocks internalization into human lung epithelial cells during the early phase of infection of influenza virus A(H1N1)/pdm09 in vitro.
But antihistamines have their own toolkit against viruses and cytokine storms:
Regarding antihistamines, in recent years molecules with antihistamine activity have been identified as having powerful antiviral properties, inhibiting the entry of certain viruses into the target cell, such as the Ebola virus (filovirus) [28], or the hepatitis C virus (flavivirus) [[29], [30], [31]], or by other mechanisms [32]. Several H1 receptor antagonists have demonstrated inhibitory properties on the production and expression of interleukins, chemokines, and other cytokines [33]. Specifically, cetirizine decreases interleukin production [34,35].
There’s a whole lot more in the paper, but right now I’m just thinking of all the times a doctor told me that antibiotics won’t help with a viral infection.
We’ve been living in an age of antivirals for years, but we didn’t know it. That probably wasn’t an accident…
The Treatment plan that saved nursing home patients
Naturally, instead of waiting for people to get sick, tested, and admitted to hospital Dr Blanco and co started treatment straight away, and even prophylactically — giving caregivers 12 vaccines. (Not!). They gave caregivers and others in the nursing home polaramine or some other equivalent before they even got sick.
Click to enlarge.
I’ve added the common brand names in brackets below.
Clinical management of COVID-19 used in the nursing homes of Yepes
1.Early start of treatment, regardless of the severity of patient symptoms.
2.Patients with mild or recent-onset symptoms (cough, fever, general malaise, anosmia, polymyalgia):
-Antihistamines every 12 h: dexchlorpheniramine (Polaramine) 2 mg, cetirizine (Zyrtek) 10 mg or loratadine (Claritin) 10 mg.
-Azithromycin 500 mg orally every 24 h for 3 days if there is rapid improvement, and for 6 days if the duration of symptoms is prolonged.
-If pain or fever, acetaminophen (Panadol) 650 mg/6–8 h.
–Nasal washing and gargling with sodium bicarbonate water (half a glass of warm water with half a teaspoon of sodium bicarbonate).
3.If symptoms of severity (dyspnea, breathing difficulty, mild or moderate chest pain, with SpO2 >80%, heart rate <100 beats per minute at any time of the process):
-Antihistamines + Azithromycin (see mild treatment management)
-Levofloxacin 500 mg/12 h, up to 14 days of antibiotic treatment from diagnosis.
-Mepifilin solution, 50 mg/8 h as a bronchodilator, until subjective improvement. Patients with previous lung disease (asthma or COPD) used their usual bronchodilators.
-If the patient experienced increased breathing difficulty, prednisone 1 mg/kg/day divided into two doses until clinical improvement, and then it was slowly tapered down.
4.Prophylactic treatment for close contacts, including all asymptomatic residents:
-Antihistamines at the same dose as symptomatic patients.
ARS-2 infects the ACE-2 receptor, which is expressed on MAST cells, which are an immune cell loaded with histamine, notorious for their role in allergic reactions.
It is only an observational study, not a randomized, blinded one, but the results are remarkable.
As always , you must check out the side effects and cross reactions with medications yourself. Polaramine is well known for making people drowsy, so don’t drive or pilot a passenger aircraft. The antibiotics need a prescription. But you may want to have some antihistamines on hand, so consider them now, before the FDA or TGA bans them. I’ll say more sometime about other antihistamines. This study was based on 90% polaramine, though other studies use the other varieties.
It was obvious this treatment plan was doomed
Listen to Dr Blanco and co:
This safe and inexpensive treatment protocol could have a crucial impact …
Antihistamines and azithromycin are drugs with extensive experience of use, good safety profile, good tolerance, low cost and wide availability, so this combined treatment regimen may respond to the global therapeutic needs for COVID-19 for all age groups. Clinical trials are necessary to determine its efficacy. As there are no commercial interests, they should be promoted by national health systems as a social responsibility.
If only. How many people might have been saved?
Hat tips here to Lance, Hanrahan, OldOzzie, Jim Barker, Vicki, and PeterC, and Antonie for prodding.
Big Protests coming up on Saturday in Perth, Brisbane, Broadbeach. Please add details in comments for other locations. I was very impressed someone put a handout with information about risks of vaccinating children in my letter box yesterday. Organised. Great to see.
Will the Greens give up their love of Apple when they hear how it effectively sold out its principles, tech secrets, and jobs to the Chinese Communist Party? Apple is the world’s biggest company, a $3 Trillion giant. Yet in order to get into the worlds biggest new market, it looks like Apple sold out the nation and the civilization that bore it.
Apple Chief Executive Tim Cook inked a $275 billion giveaway in 2016 that explains the tech company’s success in China, according to secret documents reportedly seen by
To sweeten the negotiations, Cook apparently agreed to a $1 billion investment in Didi Global, Uber’s Chinese competitor, at a critical time in the fight between the two companies for ride-hailing market shares in China. A few days later, Apple agreed to spend $275 billion in China over five years, including on what should be considered forced technology development and transfer.
According to The Information’s Wayne Ma, the deal “committed Apple to aiding roughly a dozen causes favored by China,” including “a pledge to help Chinese manufacturers develop ‘the most advanced manufacturing technologies’ and ‘support the training of high-quality Chinese talents.’”
China siphons off Western intellectual property, often with the help of the West.
First China hauled (and we gave) the factories, then it was the hi tech industry, now it’s biomedical ingenuity. The pattern repeats. China offered cheap labor for manufacturers and the tech industry with few annoying environmental burdens. Now China offers money and freedom from ethical quandaries for researchers who want to clone, create bioweapons, or hybrid human-animal cells.
As ZMan said about the biotech theft:
Most important, what we are seeing is what happens when a society decides that the value of everything is what someone will pay for it. In America, everything has a price, so nothing has value. The elites are happy to trade technology to China, because the only thing that matters is short term profit. From the Chinese perspective, the American empire is not a competitor. It is just a big candy store that she can systematically pick clean until it finally collapses. This is the war China knows it can win.
What would stop it?
If companies like Apple worried (before they sold out) that their entire brand-name would evaporate in all their current markets. If patriotism meant that all the hipster Gen Z’ers and lost corporate Millennials reacted in horror and abandoned their iphones, or the soft greens recoiled from the thought of owning a item made by a company that helped to hide Uygher slave camps?
Yet where is the media? Where are the righteous, indignant fashionistas? Is Greenpeace protesting?
Apple, Nike and Coke are all lobbying to prevent the US congress from making laws that would make it harder to get goods from Xinjiang unless companies can prove they did not use forced labor.
So Apple may think it bought a market in China, but really it paid to become a wing of the Communist Government.
According to a 2020 report from the Australian Strategic Policy Institute (ASPI), Apple is a beneficiary of Xinjiang’s forced labor transfer programs through Apple suppliers O-Film Technology and Foxconn.
We need a real media. But since we don’t have one, spread the word about Apple
It’s almost like some at the ABC are sympathetic to the anti-wind-farm movement?
The awakening begins. There is an opening here for the two opposite ends of the political debate to come together, and to figure out who the real enemy is — something that would transform the political landscape. Before anyone gets the urge to rub their noses in it (no matter how deserved it is) ponder how useful this is as a way to open a conversation. There are still good green tinted people out there who have no idea they are being used, or that there is a cheaper energy source that feeds plants, doesn’t chop up birds and bats, and doesn’t consume 13,000 hectares of wilderness either.
“I thought, ‘Geez, there’s a lot of destruction here. They’ve transformed what was a really great, pristine area … into a really industrial area’.”
Biologists don’t like it either:
According to James Cook University adjunct professor and evolutionary biologist, Dr Tim Nevard, Far North Queensland is one of Australia’s most biodiverse regions and many of the sites chosen for wind farms are “wholly inappropriate”.
“Biodiversity is the buffer at the end of the tracks that stops the runaway train of climate change from bursting through,” Dr Nevard says.
“Destroying biodiversity in order to have greater amounts of wind energy is a complete oxymoron. It’s ridiculous. So we shouldn’t be doing it.”
After Steve Nowakowski saw more wind farm applications — his opposition to them hardened. He gave a speech to locals, with photos. He thought they might throw eggs at him. Instead, none of them wanted the industrial complexes in the local wilderness either. (Imagine that?)
The Aboriginal activists were also annoyed and dismayed. The new projects in Queensland are going to be even bigger and more invasive. Some 13,000 hectares of vegetation will be removed if all the planned subsidy farms go ahead, and 90% of that land is in Queensland.
The ABC article is a long gushing feature. It ends, like a cult fanclub, with the belief that wind farms are still useful. They just need to be built somewhere better they say, as if there is plenty of land which has high wind, large transmission lines and no native fauna or farmers. But people don’t build billion dollar interconnectors to nowhere, so it’s a fantasy combination.
This is an opening in the wall to reach the soft greens. Join with them in lamenting the environmental damage, then walk them through the Valley of Vested Interests, pointing out who is really getting rich. Then gently lead them to realize that almost all the Environmental popular movements are not even trying to help the environment.
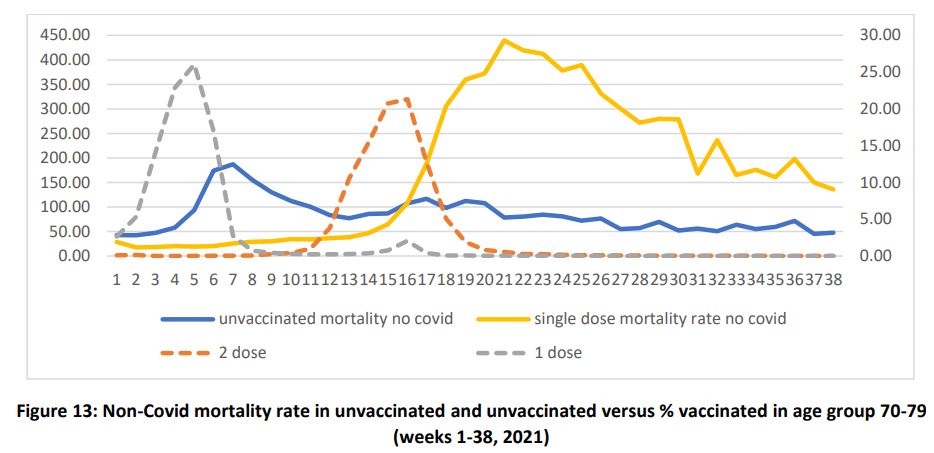
The data in the UK is some of the best in the world, but if a person has a vaccine and dies in the next two weeks, it’s classed as an “unvaccinated death”. People are not counted as fully vaccinated until 14 days after their second dose, which makes sense if we’re only looking at Covid deaths. But it doesn’t make sense when looking at other deaths. This delayed categorization leads to enigmatic effects, to say the least.
Strangely, the unvaccinated are increasingly likely to die from the week after other people in their age group get the vaccine…
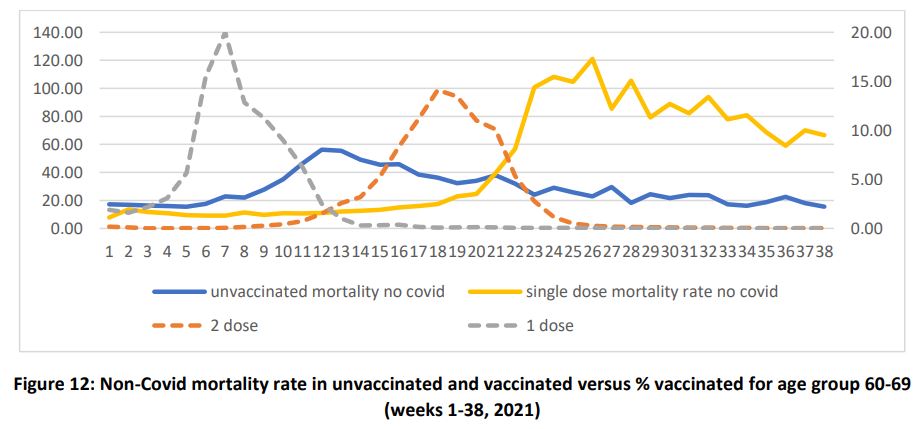
The graph below of the 70-something age group in the UK, charts the non-Covid deaths — all the heart attacks, strokes, cancer and accidents. But notice how the first dose of Covid vaccines peaked in Week 5 (the grey dashed line), but the mortality of the unvaccinated (the blue line) peaks 2 weeks later? These are the non-covid deaths, so heart attacks, strokes, all kinds of things are killing the unvaccinated two weeks after the peak in vaccination for other people in their age-group.
Most 70-somethings who did get vaccinated, got their second dose around Week 15 (orange dashed line). Just as those jabs were going in, oddly people who had only had one dose began dying at an unusually high rate (orange line), and their odd heart attacks and strokes or any cause continued for weeks through summer, a time when usually mortality rates are lower.
Strangely, the unvaccinated are more likely to die a couple of weeks after their cohort gets their first dose of the vaccine?
Norman Fenton and others at Queen Mary University of London, did these graphs, and have published a paper with many more. They think it’s very likely (what an understatement) that the mortality peaks are being misapplied to the unvaccinated and the single dose categories, when they are adverse effects from the vaccines, naturally skewing all the data on the cost-benefits and risk analysis.
It was the same in the 60 somethings:
…
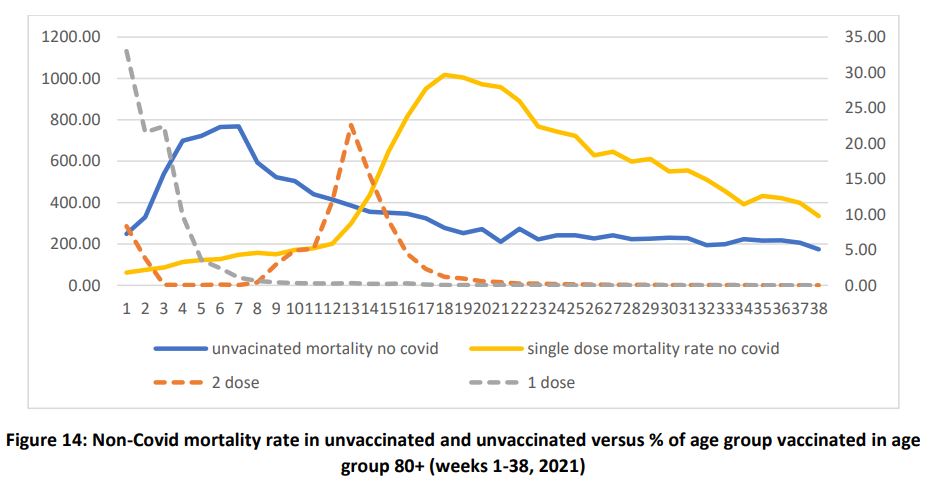
And in the older age group too: Different weeks, but same distinctive pattern:
…
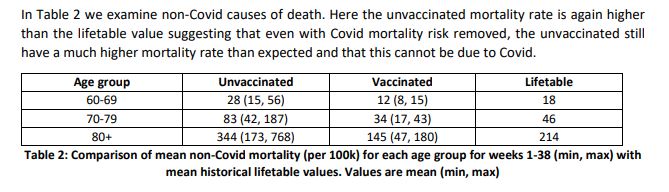
There are other mysterious anomalies. We’d expect the vaccinated to be more likely to be the higher risk, older and sicker people who are slightly more likely to die of all causes than the unvaccinated, yet the vaccinated don’t just die less often (according to the official stats) they die less often than their annuities tables suggest — less than people their age would normally die.
Consider what we are witnessing here. We have a vaccine whose recipients are suffering fewer deaths by causes other than covid and hence are benefitting from improved mortality. It appears very unlikely that this can be from the vaccine since the very best we can hope for is that the vaccine is causing no adverse reactions leading to additional non-Covid deaths. Instead, we have the unvaccinated who are suffering increased non-Covid mortality, especially in the near term close to the vaccine rollout for each age group. This is enigmatic. Does the vaccine have short-term benefits beyond reducing Covid deaths? Is undetected Covid increasing mortality in the unvaccinated in a way that presents itself as other causes of death? If so, why would it be staggered by vaccine rollout periods across age groups? None of these possible reasons make any sense so we need to look elsewhere for a more plausible explanation.
Can vaccines make people younger? Can vaccines make people who didn’t take them older?
Normally, in any given year, the things that increase deaths in 70 year olds also increase deaths in all the older ages at the same time. Instead, in every older age cohort the deaths of the unvaccinated are associated with the vaccination roll outs.
Notice that the deaths per 100,000 are much lower in the 80+ vaccinated group, than in the unvaccinated group. These are not Covid deaths. It’s like the vaccines protect vaccinees from heart attacks, but put the unvaccinated at higher risk…
Fenton, Table 2. Mortality of unvaccinated and vaccinated compared to lifetime death rates.
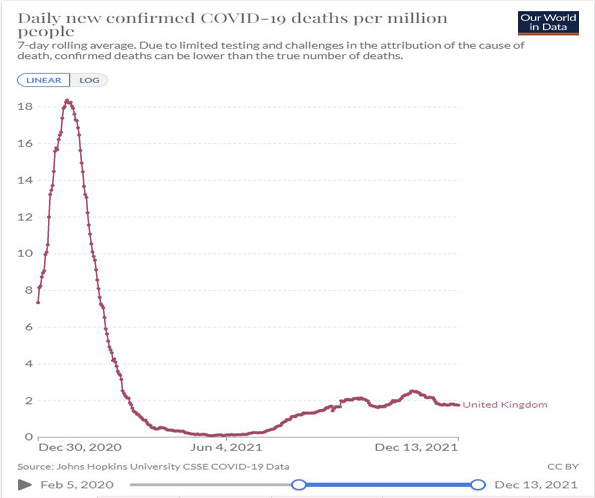
Naturally, they wondered, like I did, whether these were deaths due to Covid but in untested people. We know Covid can cause heart attacks and strokes, and we know the UK missed a lot of cases. But most of those missed deaths would have been in the first weeks of the year, and not during summer.
UK Covid deaths peaked in January, which would likely also be when undiagnosed Covid deaths peaked too. | Source: OWID
It’s worth bearing in mind, despite these rather shocking graphs that there is no overall excess deaths from vaccines in the UK compared to other years. Excess deaths always has a wide margin of normal variation, so less deaths from influenza leaves room for more deaths in other areas, so to speak:
The scale of the mortality adjustment suggests that approximately 14% of all deaths are being miscategorised across all three age groups.
In line with the fact that the data does not reveal excess mortality compared to previous years, we see no direct evidence of overall excess mortality caused by vaccine side effects in the data. The spikes in mortality that appear to occur soon after vaccination may be caused by the infirm, moribund, and severely ill receiving vaccination in priority order and thus simply appearing to hasten deaths that might otherwise have occurred later in the year
What I like about this paper is that it’s so professionally written, and that, Fenton et al, work hard to find other reasons to explain these strange patterns. They consider all the ideas offered by the ONS (Office of National Statistics) and others, and rule out that the unvaccinated were significantly more likely to be ethnic groups who have higher mortality, or terminally ill people who couldn’t be bothered getting vaccinated on deaths door, or that a more virulent strain appeared, or that the deaths in the “single dose” group were the people who were too sick for some other reason to get their second dose.
Why was this data not available before?
Incredibly, despite this being a national emergency, data was not split into separate age groups until recently “Week 44”, whereby these very odd patterns show up. Since age is the single most important variable in any Covid data, and the highest risk factor for death, this lack of data seems inexcusable. It’s baffling that those aged 10 – 59 are still bundled together, a worthless blurred conglomerate of people of both high and low risk. Where are those separate age cohorts? We need to see them…
The adverse effects:
Fenton et al suspect some of the adverse effects of the vaccine may be occurring in people who catch Covid either just before, or just after getting vaccinated. If that’s the case, we ought not have that in Australia, at least in some states where vaccination programs have gone out with no Covid present at all. Given the rush to push boosters now, surely understanding the risks would be priority number one, so we could reduce them?
But few in the Ministry of Health seem too concerned about our actual health.
The bottom line:
Covid vaccines don’t seem to prevent deaths overall. That surely changes the risk-benefit equation. If there is an advantage in getting vaccinated against Covid, it is seemingly offset by the side effects of taking Covid vaccines.
Thanks to Custer van Cleef. Prophet of Boom. Paul Cottingham. David E. OriginalSteve




















{kind=link}
{kind=link}
{kind=link}
Recent Comments