Blockbuster Review papers like this are very useful to pass on to your doctor or officials. And until all patients get some synopsis of this or equivalent, there is no informed consent.

Dr Aseem Malhotra
As Dr Aseem Malhotra says: “It’s perhaps the most important work of my career so far…”
The great thing is that he is speaking at medical conferences in the UK, and senior doctors are astonished. There is hope that things may yet improve after the worst medical experiment in history.
The figures that hit the hardest are that for the young, thousands of people need to be vaccinated to save one life, yet in the UK 1 in 120 people suffer from something defined as more than mild effects, and in Norway 1 in 1,000 end up in hospital or with “life changing” effects.
Dr Malhotra was the cardiac specialist I wrote about in November last year, who put forward the first very convincing case I had seen that not only were cardiac inflammatory risk factors doubled after vaccination (Gundry et al) which might double the risk of heart attacks, but that reports and images of cardiac damage and an increase in heart attacks in the UK were being actively suppressed for fear that the researchers would lose grant money if they published them.
Yet he had started off supporting the mRNA vaccines. In January 2021 he was one of the first to get the Pfizer vaccine in the UK, and was interviewed on Good Morning Britain to promote the vaccine. It was only after his father died unexpected from a heart attack in July 2021, with inexplicable levels of blockages, that he started to change his mind. Despite being a cardiac specialist, and he could not explain his fathers death. It didn’t fit the risk patterns he knew. It would take him months of investigation to “slowly and reluctantly” conclude the vaccines were “far from being safe and effective”. His father, by the way, was Dr Kailash Chand OBE, 73, and former deputy chair of the British Medical Association (BMA). He was very fit and healthy until his sudden death in the months following his second Pfizer dose.
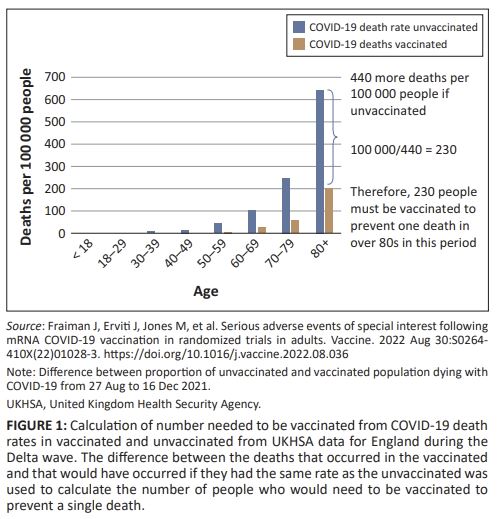
This week Dr Malhotra has published a full review of the known risks and benefits, and the numbers are damning. Even in people in their 80s, as many as 230 people people need to be vaccinated to prevent one death — and that was with the Delta variant during 2021, when vaccines were more useful and before the Omicron variant arose to escape them. For people in their fifties, at least 2,600 of the cohort would have to vaccinated to save one life. For those in their twenties, at least 93,000 would need an injection to save one. In 2022 with Omicron, all these numbers would be much higher.
And this of course is not to count the risks, just the benefits.
…
But the harms, the harms!

Ambulances were called out 20% more than normal for cardiac arrests after the vaccination program started. Something bad was going on.
It is instructive to note that according to ambulance service data, in 2021 (the year of the vaccine roll-out), there were approximately an extra 20,000 (~20% increase) out-of-hospital cardiac arrest calls compared to 2019, and approximately 14,000 more than in 2020. Data obtained under Freedom of Information laws from one of the largest ambulance trusts in England suggest that there was no increase from November 2020 to March 2021, and thereafter the rise has been seen disproportionately in the young. This is a huge signal that surely needs investigating with some urgency.
There was a 25% increase in heart problems in 16 – 39 year olds — linked to the vaccine, not to Covid:
Similarly, a recent paper in Nature revealed a 25% increase in both acute coronary syndrome and cardiac arrest calls in the 16- to 39-year-old age groups significantly associated with administration with the first and second doses of the mRNA vaccines but no association with COVID-19 infection.
Myocarditis may not be fatal very often, but it leaves some permanent heart damage and we don’t know what this will mean 40 or 50 years in the future. Reports of myocarditis ranged from 1 in 6000 in Israel to 1 in 2700 in a Hong Kong study in teenage boys. Clearly far more teenagers were harmed rather than saved:
Although vaccine-induced myocarditis is not often fatal in young adults, MRI scans reveal that, of the ones admitted to hospital, approximately 80% have some degree of myocardial damage. It is like suffering a small heart attack and sustaining some – likely permanent – heart muscle injury. It is uncertain how this will play out in the longer-term, including if, and to what degree, it will increase the risk of poor quality of life or potentially more serious heart rhythm disturbances in the future.
In the UK reports of side effects suggest as many as 1 in 120 people suffered an effect that was more than mild. This was 30 times higher than side effects reported for the MMR (Measles Mumps Rubella) vaccine. In Norway, perhaps the most shocking of all, as many as 1 in 1,000 people suffered severe effects — things that were bad enough to put them in hospital, or things that were “life changing”.
In the United Kingdom, since the vaccine roll-out there have been almost 500 000 adverse event reports recorded (via the Yellow Card system) in association with the mRNA COVID-19 vaccinations involving over 150 000 individuals. In terms of the number of reports per person (i.e. having received at least one dose), the MHRA figures show around 1 in 120 suffering a likely adverse event that is beyond mild. [Yellowcard, UK Gov] However, the MHRA are unclear about the rate and furthermore do not separate out the serious adverse events. Nevertheless, this level of reporting is unprecedented in the modern medical era and equals the total number of reports received in the first 40 years of the Yellow Card reporting system (for all medicines – not just vaccines) up to 2020.33 In comparison, for the measles, mumps and rubella (MMR) vaccine, the number of reports per person vaccinated was around 1 in 4000, more than thirty times less frequent than the 1 in 120 Yellow Card reports for COVID-19 vaccine recipients. Norway does separate out the reported serious adverse reactions and has shown a rate of approximately 1 in 1000 after two doses of BioNTech/Pfizer mRNA product that result in hospitalisation or are life changing. [Norwegian Medicines Agency].
In the US 24,000 people are known to have died, and one third of those were within just 48 hours of vaccination.
As with the UK’s system, the level of reports – including serious ones – associated with COVID-19 vaccines is completely unprecedented. For example, over 24000 deaths have now been recorded in VAERS as of 02 March 2022; 29% of these occurred within 48 h of injection, and half within two weeks. The average reporting rate prior to 2020 was less than 300 deaths per annum.
But how many died four to 12 weeks later, or longer, and were not reported or not even considered to be associated with a vaccination risk? Estimates of under-reporting suggest in the UK that only 10% of adverse effects are officially logged, and in the US it may only be 1%.
Injecting a pathogenic spike…
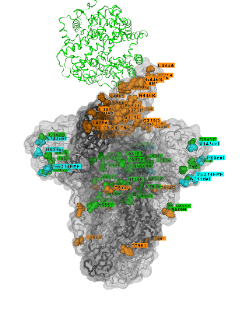 Dr Malhotra notes that the spike is produced for at least four months, spreads widely through the body but was not an inert protein at all. It was the source of the damage to the vascular system and lungs that Covid caused.
Dr Malhotra notes that the spike is produced for at least four months, spreads widely through the body but was not an inert protein at all. It was the source of the damage to the vascular system and lungs that Covid caused.
For the COVID-19 vaccines, spike protein has been shown to be produced continuously (and in unpredictable amounts) for at least four months after vaccination and is distributed throughout the body after intramuscular injection. For the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines, the spike protein was chosen, possibly because it enables cell entry. However, this protein is not inert, but rather it is the source of much of the pathology associated with severe COVID-19, including endothelial damage, clotting abnormalities and lung damage.
The bottom line is that during a seemingly deadly pandemic, we should have seen some benefit overall from mass vaccination yet we don’t:
It would be surprising – to say the least – if during an apparently deadly pandemic, an effective vaccine could not clearly and unequivocally be shown to reduce all-cause mortality.
All cause mortality is one of the hottest clues in the world of medical research world, because it captures effects we weren’t looking for. Dr Malhotra quotes the Neil and Fenton study on all cause mortality that I described last December. It’s the spooky and very well done study that suggested the unvaccinated are increasingly likely to die in the weeks after other people in their age group get the vaccine. It was a kind of lightning rod effect that was an artifact of calling people “unvaccinated” for two weeks after their vaccine dose. (Notably that two week period is when half of those deaths due to vaccination occurred in the US VAERS database.)
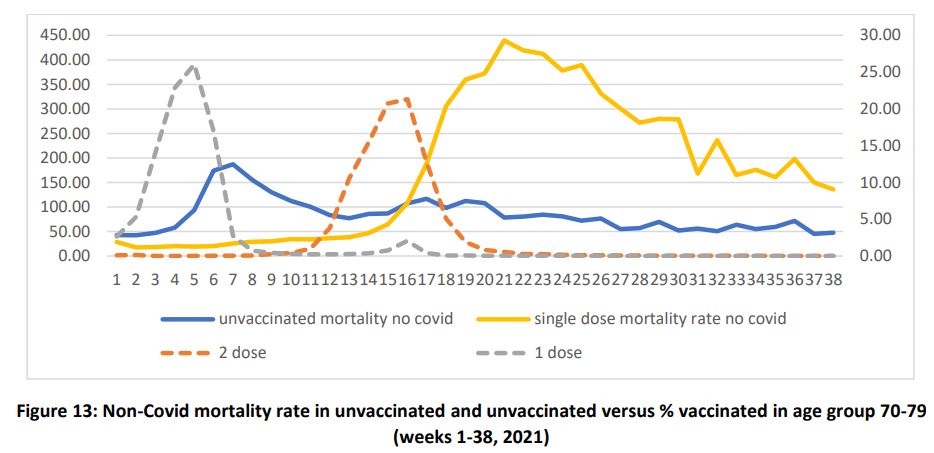
Strangely, the unvaccinated are increasing more likely to die in the week after the first dose peaks in their age group.
Dr Malhotra is also talking about the dark influence of Big Pharma and the desperate need to redesign the entire medical system (more on that another day).
Word is getting out. Inexcusably, unforgivably, slowly.
REFERENCE
Aseem Malhotra, (2022) Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine – Part 1, Journal of Insulin Resistance, ISSN: (Online) 2519-7533, (Print) 2412-2785
Gundry, Steven (2021) Mrna COVID Vaccines Dramatically Increase Endothelial Inflammatory Markers and ACS Risk as Measured by the PULS Cardiac Test: a Warning. 8 Nov 2021 Circulation. 2021;144:A1071. ONLY a Preprint ABSTRACT.
Norwegian Medicines Agency. (2022) Reported suspected adverse reactions to COVID19 vaccines as of 04.01.2022 [cited 2022 May]. PDF
UK Government: Coronavirus vaccine – Weekly summary of Yellow Card reporting [homepage on the Internet]. GOV.UK. [cited 2022 Jun 5]. Available from: UK Gov
Neil, and Fenton et al (2021) Latest statistics on England mortality data suggest systematic mis-categorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination
Covid-19 vaccine and syringe against Biontech and Pfizer logos by Marco Verch under Creative Commons 2.0
and the Vaccine Spike from GisAID